Surgical prevention of terminal neuroma and phantom limb pain: a literature review
Article information

Abstract
The incidence of extremity amputation is estimated at about 200,000 cases annually. Over 25% of patients suffer from terminal neuroma or phantom limb pain (TNPLP), resulting in pain, inability to wear a prosthetic device, and lost work. Once TNPLP develops, there is no definitive cure. Therefore, there has been an emerging focus on TNPLP prevention. We examined the current literature on TNPLP prevention in patients undergoing extremity amputation. A literature review was performed using Ovid Medline, Cochrane Collaboration Library, and Google Scholar to identify all original studies that addressed surgical prophylaxis against TNPLP. The search was conducted using both Medical Subject Headings and free-text using the terms “phantom limb pain,” “amputation neuroma,” and “surgical prevention of amputation neuroma.” Fifteen studies met the inclusion criteria, including six prospective trials, two comprehensive literature reviews, four retrospective chart reviews, and three case series/technique reviews. Five techniques were identified, and each was incorporated into a target-based classification system. A small but growing body of literature exists regarding the surgical prevention of TNPLP. Targeted muscle reinnervation (TMR), a form of physiologic target reassignment, has the greatest momentum in the academic surgical community, with multiple recent prospective studies demonstrating superior prevention of TNPLP. Neurorrhaphy and transposition with implantation are supported by less robust evidence, but merit future study as alternatives to TMR.
INTRODUCTION
The incidence of extremity amputation is estimated at 200,000 cases annually [1,2]. Of these, over 25% suffer from terminal neuroma or phantom limb pain (TNPLP), resulting in intractable pain, inability to wear a prosthetic device, and lost work [3,4]. Due to the significant disability generated by TNPLP, it is an area of growing scientific interest and investigation.
Despite a large body of literature on the management of established TNPLP, treatment outcomes remain unpredictable [4-28]. A convincing body of neuroscience literature supports the concept of cortical reorganization and the imprinting of peripheral pain onto the central pain centers [29-47]. This central maladaptation may explain the unpredictability of peripheral treatment of established TNPLP. The clinical and basic science data support a transition in approach from the treatment of established TNPLP to its prevention.
Both non-surgical and surgical preventative approaches have been explored. The results of pharmacological and physical therapy strategies for the prevention of TNPLP are unfortunately disappointing [27,48-65]. On the contrary, though small in number, TNPLP surgical prevention strategies have shown great success.
The purpose of this literature review is to evaluate the current body of literature on surgical techniques for the prevention of TNPLP in patients undergoing extremity amputation, and secondarily to propose a new target-based classification system for the surgical prevention of TNPLP
METHODS
Search strategy
An online search was performed using Ovid Medline, Cochrane Collaboration Library, and Google Scholar to identify all original articles that addressed surgical prophylaxis against TNPLP. The following search terms were used: “phantom limb pain,” “amputation neuroma,” and “surgical prevention of amputation neuroma.” The search was limited to articles in English from inception to 2019. Studies regarding non-surgical strategies, animal studies, or surgical strategies for the treatment of established neuroma or phantom limb pain were excluded. After removal of all duplications, citations from all three search engines were subjected to title and abstract screening by two independent reviewers (RNB and SBC). The full-text articles of studies that met the inclusion criteria were subsequently obtained and reviewed independently by two reviewers. Disagreement in data collection was resolved by consensus with a third evaluator (BNNT).
Data collection
The final list of studies was independently evaluated by two independent reviewers (RNB and SBC) and the following variables were extracted: article identifiers, technique category, purpose, design, sample size, analysis techniques, quantitative results, strengths, and limitations. The original two researchers independently reviewed each article and compiled their own tables. These were then combined and submitted to the principal investigator for final review.
Classification of techniques
A recent literature review introduced a classification system for surgical prophylaxis against TNPLP, according to which techniques are divided into the categories of end closure, transposition with implantation, neurorrhaphy, and alternate target reinnervation [11]. We proposed the addition of a new category, preservation of continuity, and subsequently re-categorized these approaches based on the target condition to ensure consistent terminology throughout the review. We opted to rename “alternate target reinnervation” as “targeted muscle reinnervation” due to the increasing prevalence of the latter term in the literature. The proposed target-based classification system, which is shown in Fig. 1 and demonstrated in Fig. 2, includes the target deficient, target reassignment, and target in continuity techniques.
Flow diagram.
Schematic of techniques. TMR, targeted muscle reinnervation; RPNI, regenerative peripheral nerve interface; TNI, targeted nerve implantation.
Target deficient
In this category, the severed nerve is not coapted to another nerve. Rather, the severed nerve ending is closed off or buried. Transposition with implantation is a common strategy in which terminal nerves are buried into muscle, bone, or fascia so that their nerve endings grow into stable, deep structures rather than exposed pain receptors in the skin [11]. The end closure technique refers to manipulation of the epineurium to enclose the nerve’s fascicles.
Target reassignment
In target reassignment, a severed nerve is coapted to a new nerve to provide natural ingrowth within a nerve sheath. This can be physiologic or non-physiologic, as described below.
In physiologic target reassignment, the proximal severed nerve is coapted to a distal nerve attached to an end organ with its normal peripheral nerve endings. This theoretically provides the severed nerve with a normal end organ to grow into, reducing the changes of TNPLP.
The most popular version of this technique is known as targeted muscle reinnervation (TMR). TMR is the coaptation of proximal, terminal mixed nerves to distal, end motor nerves, providing a distal target for regenerating terminal axons. Notably, the distal, end motor nerve, once transected, intrinsically leads into a denervated segment of muscle, which is posited to attract physiologic nerve ingrowth into the muscle. TMR was developed for the purpose of creating functional electromyogram signals for integrated, controllable prosthetic devices [6,28]. Similarly, targeted nerve implantation (TNI) is the coaptation of proximal, terminal mixed nerves into distal motor nerves solely for the purpose of neuroma prevention [15].
An exception to the above definition is the regenerative peripheral nerve interface (RPNI) technique. In RPNI, a severed nerve is implanted directly into a non-vascularized muscle graft. This denervated muscle graft provides the severed nerve with an end organ to grow into in a physiologically natural way [21,66]. This theoretically reduces the risk of TNPLP. Like TMR, this reinnervation has been demonstrated by electromyogram signals.
In non-physiologic target reassignment, two proximal severed nerves are coapted, or a single nerve is split and coapted to itself. While these techniques provide a nerve sheath for axon ingrowth, they do not lead to a physiologic, distal end organ. These techniques are termed neurorrhaphy. Centro-central union (CCU) is an analogous term commonly found in the literature [5,67].
Target in continuity
These techniques can only be utilized when intermediate extremity components are amputated, while the proximal and distal tissues are preserved. Target in continuity techniques preserve the continuity of nerves and blood vessels to the terminal end organs, so that the amputation defect is reconstructed by the intact, distal parts. This category includes preservation of continuity, rotationplasty, and “spare parts” free tissue transfer.
Preservation of continuity is most frequently described for interphalangeal joint amputations of the digits. In this technique, the distal pulp, connected to the neurovascular bundles, is transposed proximally and sewn to the proximal amputation stump after removal of the intervening tissues. Thus, the wound is reconstructed with robust, vascularized, and innervated tissue. In this technique, the proper digital nerves are never severed; theoretically, there is no opportunity for neuroma formation [68,69].
Rotationplasty of the lower limb is a procedure in which the knee is amputated, and the foot and ankle are rotated 180° and reattached proximally. The tibia is fixated to the femur so that the reversed ankle joint acts as a pseudo-knee, allowing the transfer of power through a specialized prosthetic device.
Another strategy is the use of “spare parts,” or a fillet flap to cover an amputated part. This technique may be used in the setting of trauma, where only some of the distal tissues are viable and useful for reconstruction—usually to preserve the length of the traumatized extremity. The distal tissues are dissected, maintaining their connections to arteries and veins. This fillet flap is transferred to the wound and the blood vessels are then anastomosed. The nerves can be coapted surgically to prevent future neuropathic wounds and, theoretically, to prevent TNPLP.
RESULTS
The Ovid Medline search returned 425 PubMed-indexed articles, from which only 10 articles met the inclusion criteria. The Cochrane Library database search produced 170 articles. No Cochrane Reviews on the topic exist and none of the articles met the inclusion criteria. The Google Scholar search produced 431 articles, from which one article met the inclusion criteria. There were four other articles that were found by reference searching. A total of 15 articles met the inclusion criteria and are summarized in Table 1.
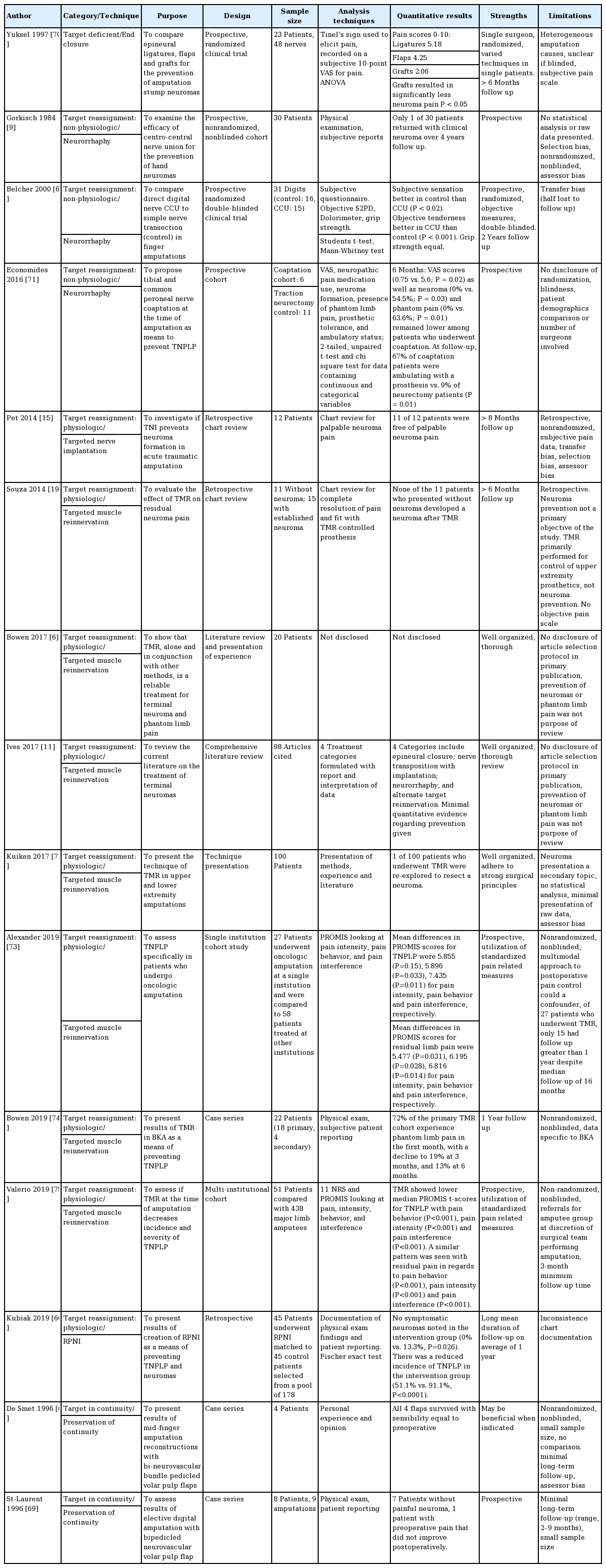
Summary of articles meeting the inclusion criteria on the surgical prevention of terminal neuroma and phantom limb pain
There was one study on the target deficient technique (end closure, n=1), 12 studies on target reassignment (physiologic TMR, n=8; RPNI, n=1; TNI, n=0; non-physiologic neurorrhaphy/CCU, n=3), and two studies on target continuity (preservation of continuity, n=2; rotationplasty, n=0; fillet flap, n=0). There were six prospective trials, two comprehensive literature reviews, four retrospective chart reviews, and three case series/technique reviews.
Target deficient
This literature review identified no studies evaluating the use of transposition with implantation in the prophylactic setting. A single article by Yuksel et al. [70] testing the end closure technique met the inclusion criteria. Yuksel et al. performed a prospective, randomized clinical trial including 23 patients and 48 nerves to compare epineural ligatures, flaps, and grafts for the prevention of amputation stump neuroma. The Tinel sign was used to elicit pain, which was recorded on a subjective 10-point visual analog scale for pain. The grafts, applied by excising a piece of epineurium and suturing it over the terminal nerve, demonstrated the greatest reduction in pain, with a pain score of 2.06 compared for 5.18 for ligatures and 4.25 for flaps (P<0.05). In summary, this study utilized the residual epineurium in three different ways and subjectively compared the prevention of neuroma formation. While grafts performed best, none of the techniques demonstrated excellent control [70]. This study had several limitations, including heterogeneous amputation causes, no clear statement of whether the study was blinded, the use of a subjective pain scale, and no histological confirmation of results.
Target reassignment
Non-physiologic target reassignment
This review identified three studies evaluating neurorrhaphy or CCU in the preventative setting. A nonrandomized, nonblinded, noncomparative prospective cohort study by Gorkisch et al. [9] in 1984 examined the efficacy of CCU for the prevention of hand neuroma. This group reported strong, albeit subjective results of this technique, with only one of 30 patients returning with clinical neuroma over a 4-year follow-up period.
Belcher and Pandya (2002) [67] performed a prospective, randomized, double-blinded clinical trial comparing CCU to simple transection in digital nerves. While half of the patients were lost to follow-up, objective tenderness measures demonstrated significant superiority of CCU (P<0.02).
Economides et al. (2016) [71] performed a small, prospective pilot study comparing tibial and common peroneal neurorrhaphy with collagen wrapping to nerve transection. This study demonstrated the superiority of CCU in multiple subjective and objective outcomes including the Tinel sign (P=0.03) and ambulation with a prosthetic device (P=0.01).
Physiologic target reassignment
There were nine articles on physiologic target reassignment techniques, with TMR being the most prominent area of study (n=7), followed by RPNI (n=1) and TNI (n=1).
Souza et al. (2014) [19] performed a retrospective chart review evaluating the effect of TMR on 11 patients without terminal neuroma and 15 patients with established terminal neuroma. None of the 11 patients who presented without neuroma developed a neuroma after TMR.
Bowen et al. (2017) [6] performed a comprehensive literature review and presentation of their experience with TMR as a reliable treatment for TNPLP. In a further prospective study in 2019 by Bowen et al. [74], 22 patients underwent TMR at the time of below-knee amputation and none of the patients reported neuroma pain postoperatively. While no numerical measures were provided, the authors disclosed that a clinical trial underway at their institution showed encouraging results of TMR for the prevention of TNPLP.
Ives et al. (2017) [11] performed a comprehensive literature review on the treatment of terminal neuroma. These authors developed the categorization system that was modified for use in this review. Their study investigated TMR and RPNI. Both techniques were described as promising procedures to reduce the incidence of terminal neuroma.
Kuiken et al. (2017) [72] presented methods, experiences and a review of the literature on TMR in upper and lower extremity amputation. One hundred patients were analyzed, and only one was re-explored for neuroma resection. While neuroma prevention was a secondary topic and no statistical analysis was presented, the authors mentioned TMR as a promising, albeit experimental, technique for prevention of terminal neuroma.
Alexander et al. (2019) [73] performed a prospective study assessing TNPLP among patients who specifically underwent TMR with concurrent oncologic amputations. The study measured post-amputation pain using the Patient-Reported Outcomes Measurement Information System (PROMIS) and evaluated pain intensity, pain behavior, and pain interference. Although the article did not include specific surgical techniques, the authors referenced prior works [76-78]. The authors demonstrated that patients who underwent concurrent TMR had lower incidence rates of TNPLP and residual limb pain than patients who did not undergo concurrent TMR. The mean differences in PROMIS scores for TNPLP were 5.855 (P=0.15), 5.896 (P=0.033), and 7.435 (P=0.011) for pain intensity, pain behavior, and pain interference, respectively. Meanwhile, the mean differences in PROMIS scores for residual limb pain were 5.477 (P=0.031), 6.195 (P=0.028), 6.816 (P=0.014) for pain intensity, pain behavior, and pain interference, respectively.
Similarly, Valerio et al. (2019) [75] performed a prospective study assessing TNPLP in patients who underwent TMR at the time of amputation versus those who only had amputation using the PROMIS scoring system. Their study demonstrated that those who underwent concurrent TMR had significantly lower median PROMIS t-scores (P<0.001) for TNPLP with regard to pain behavior, pain intensity, and pain interference. Likewise, a similar pattern was seen with residual pain in regard to pain behavior, pain intensity, and pain interference.
The only study examining the prevention of TNPLP using RPNI at the time of amputation was that by Kubiak et al. in 2019 [66]. The authors reported a significantly lower incidence of postoperative TNPLP and symptomatic neuroma in this retrospective study. Specifically, the authors found that six control patients developed symptomatic neuroma, while the TMR group had no symptomatic neuroma cases (P=0.026). Furthermore, 41 control patients reported TNPLP, whereas only 23 patients in the TMR group did so (P<0.0001).
Pet et al. (2014) [15] performed a retrospective chart review to investigate whether TNI prevents neuroma formation in acute traumatic amputation. Eleven of 12 patients were free of palpable neuroma pain. Despite the retrospective nature of this study, the authors concluded that TNI is a promising technique for the prevention of terminal neuroma.
Target in continuity
There were only two older studies (published in 1996) addressing the efficacy of preservation of continuity in TNPLP prevention [68,69]. The indications for this technique are limited to pathology that necessitates segmental amputation of a limb, but spares intervening neurovascular tissues. When the intermediate extremity is amputated and the proximal and distal ends are reattached with their neurovascular connections intact, the intact nerves should provide no opportunity for the development of TNPLP.
A case series of four patients who underwent neurovascular bundle pedicled volar pulp flaps for mid-finger amputation was presented by De Smet in 1996 [68]. All four flaps survived with sensibility equal to the preoperative status and no neuroma formation.
In the same year, St-Laurent and Duclos [69] presented a case series of eight patients who underwent the same procedure. Seven of those eight patients did not develop painful neuroma. The patient who reported pain suffered from preoperative pain that did not improve after surgery. We have termed this technique “preservation of continuity.”
DISCUSSION
Post-amputation TNPLP results in significant patient disability and an economic burden on the healthcare system. Although a myriad of treatment strategies, both non-surgical and surgical, have been studied and implemented, their success has been limited. In contrast, the surgical prevention of TNPLP at the time of primary amputation, although it has not been well defined in the literature, has shown the greatest potential for reducing the incidence of this debilitating condition.
To our knowledge, this is the first literature review of the surgical prevention of TNPLP and the first attempt at formulating a target-based algorithm to describe the current trends (Fig. 3). Despite the paucity of high-quality literature on the surgical prevention of TNPLP, all studies have shown promising results and affirmed the need for a more vigorous investigation of this paradigm.
A target-based algorithm for terminal neuroma and phantom limb pain surgical prevention terminology.
Target deficient
End closure may provide a simpler technique; however, it does not follow the theoretical trends towards providing an end organ for nerve ingrowth and does not have strong support from the literature. Transposition with implantation into bone, muscle, or fascia is a well described and widely utilized method for the treatment of established neuroma [7,79-83]. Surprisingly, this literature review identified no studies evaluating the use of transposition and implantation in the primary, preventative setting. Future studies on transposition with implantation would be a logical step towards the pursuit of an efficient, effective strategy to prevent TNPLP.
Physiologic target reassignment
Within the last 6 years, a rapid proliferation in information on TMR, TNI, and RPNI reflects momentum in this area, especially TMR. Multiple high-quality respective cohort studies utilizing standardized pain scales (NRS [numerical rating scale] and PROMIS) have demonstrated statistically significant superiority of TMR and TNI for surgical prophylaxis against TNPLP over no nerve interventions [73-75].
Non-physiologic target reassignment
According to our review, neurorrhaphy has demonstrated good outcomes and should be considered in most cases when more complex techniques are unable to be performed. While this technique has a moderate learning curve, it can be performed under loupe magnification and, once routine, may be performed quickly. Future prospective trials may confirm the results of the current, low-powered studies [9,67,71].
Target in continuity
This review did not identify any studies evaluating the incidence of TNPLP after rotationplasty or fillet flap, both of which have been shown to improve quality of life, prosthetic usage, functional outcome, and emotional well-being in oncologic patients [84-95].
Our 15 studies spanned 3 decades, indicating plastic surgeons’ early recognition of the debilitating impact of TNPLP on patient quality of life and, consequently, the need for prevention. Earlier studies emphasized end closure, preservation of continuity, and neurorrhaphy/CCU, whereas TMR has been the mainstay of interventions in the past 5 years. As expected, early studies were mainly case series, technique reviews, and retrospective reviews of single-surgeon experiences, whereas later studies were prospective trials involving multiple surgeons and sometimes institutions. The later trials also employed more standardized data reporting tools, as well as validated patient-centered variables such as the PROMIS score.
Our algorithm maintains previous terminology and organizes each strategy into target-based categories. This may help to guide future academic and clinical analyses of the topic. This target-based algorithm may also guide treatment based on each patient’s individual anatomy and the nerve targets that the patient offers.
CONCLUSIONS
In conclusion, this literature review demonstrates a small, yet growing body of literature on the surgical prophylaxis of TNPLP. The strongest body of literature favors the physiologic target reassignment techniques of TMR and TNI. Neurorrhaphy and transposition with implantation are supported by less robust evidence, but merit future study as simpler alternatives.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Author contribution
Conceptualization: RN Bogdasarian, SB Cai, A Ignatiuk, ES Lee. Data curation: RN Bogdasarian, BNN Tran. Formal analysis: RN Bogdasarian, SB Cai, BNN Tran. Methodology: RN Bogdasarian, SB Cai, A Ignatiuk, ES Lee. Project administration: RN Bogdasarian, SB Cai. Visualization: RN Bogdasarian, SB Cai, BNN Tran. Writing - original draft: RN Bogdasarian. Writing - review & editing: RN Bogdasarian, BNN Tran.